What’s on this page:
Access to the validation papers behind the mTBI biomarker and clinical resources for the ED physician.
Clinical Practice
Suggested algorithm for the use of mTBI in the emergency department: Suggested algorithm for the use of mTBI in the emergency department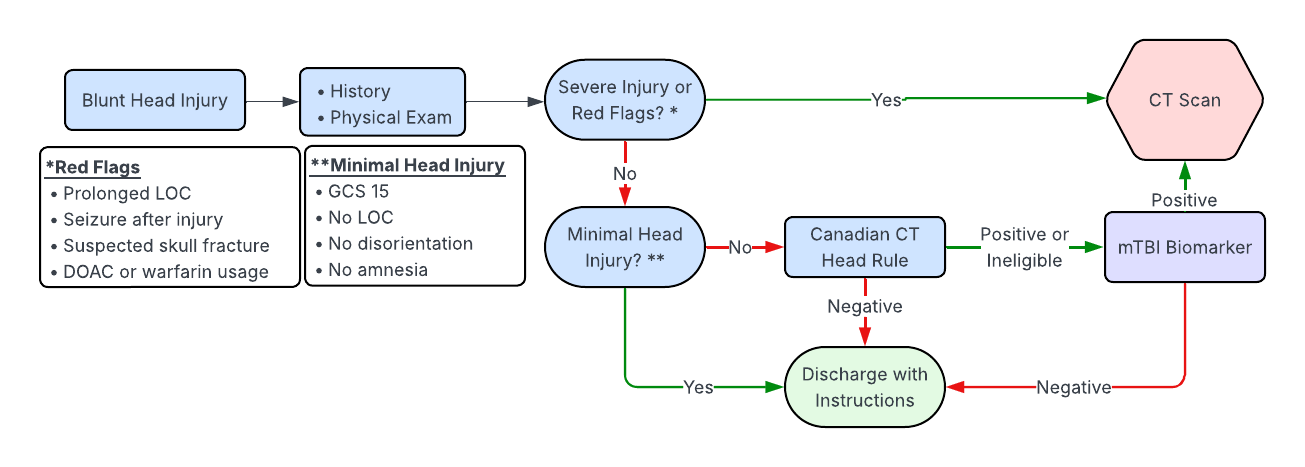
- FAQ for Clinicians — 9 commonly asked questions about the mTBI biomarker. PDF
- European Consensus Paper — Guidelines produced by a panel of experts with consensus recommendations. PDF
- Summary Slide of Implementation Goals — Brief summary slide of Edmonton specific goals for reduction of transportation for CT heads after TBI. PDF
Validation Papers
- Papa et al. (2016) — 584 patients. GFAP performed consistently in detecting MMTBI, CT lesions, and neurosurgical intervention across 7 days. UCH-L1 performed best in the early postinjury period. PDF (JAMA Neurology)
- Yue et al. (2019) — 450 patients. Measuring blood GFAP with a point-of-care test within 24 hours of injury can help detect TBI and flag patients who need imaging or follow-up. PDF (Lancet Neurology)
- Bazarian et al. (2021) — 1936 patients. In over 1,900 patients with mild TBI, the biomarker showed very high sensitivity (~96%) and negative predictive value (>99%) for detecting CT-positive brain injuries. PDF (Academic Emergency Medicine)
- Menditto et al. (2024) — 234 patients, mean age 81 years old. Patients were included even if taking a DOAC or warfarin. GFAP had a 100% negative predictive value. PDF (Clin Chem Lab Med)
- Welch et al. (2025) — 1899 patients, age 18-98 years old with head injury and GCS 9-15 in ED. Sensitivity 96.7%, negative predictive value 99.4%. PDF (American Journal of Emergency Medicine)
- Puravet A et al. (2025) – Systematic review of 16 articles on the topic (7828 patients). the combined use of GFAP and UCH-L1 demonstrates a sensitivity of 100% in ruling out intracranial injury in adults. Potentially reduce unnecessary CT scans by 31%. PDF (Annals of Emergency Medicine)
- Implementation questions: skobleni@ualberta.ca